



December in Covidlandia
A capstone article celebrating a pretty good year


Welcome back to some monthly highlights from a place I call Covidlandia, a forgotten land between black and white, carefree and cautious, pandemic beginning and end. Here I present recent news, scientific discoveries, and medical knowledge that caught my attention and that is of interest to primary care. This is a very special issue! It marks the completion of a whole year’s effort. Included you will find a case report of my first Covid illness last month, and how I treated that. No big surprises, just promises kept. We will briefly review 15 studies together. I’m trying out a more reader-friendly, slightly less technical language than usual. You’ll find a downloadable 7 page booklet synthesizing all I’ve learned, affirmed, and presented in Covidlandia for 2024 (PDF format, and feel free to share it). And finally, I’m posting a gallery of the custom artwork contributed by the 13 year old Artist-in-Residence for this year’s series. Her grandmother is also a talented artist, imparting her skills and techniques, so I thought I would share one of her works above, too. As a Pennsylvanian, this painting conjures early winter for me, and Andrew Wyeth.
Is Covid all figured out? I wish it were, but it’s not. That’s why I keep curating and commenting, but I realize that one human being cannot possibly keep up with everything. And yet I try to collect useful, actionable stuff. January, February, March, April, May, June, July, August, September, October, November, and now December.
I know that citizens of Covidlandia also appreciate the related threats of H5N1 bird flu, anti-vaccination agendas, anti-science leadership, and the resurgence of diseases like polio, whooping cough, and measles. Lessons have been learned. We also note that group fictions like “masks don’t work” are tragic, binary reductionisms, intended to enforce order and conformity at the expense of truth. God forbid another pandemic starts and we are still bickering about stupid stuff. You can expect a Covidlandia update every 1-2 months in 2025, with some expanded heads up as needed.
An excerpt from the 2024 year in review PDF that is available towards the end of this post: It is important to acknowledge how the game has changed. While Covid is still killing an average of 1,000 Americans a week through 2024, with significantly more indirectly, it is not spilling out of packed hospitals. The average person can absolutely expect to survive an infection. We also have designer vaccines, antivirals, good quality masks, and almost five years of knowledge and science as shields. The players in the game also need to be considered. Older people, the immunocompromised, the very young, and those with significant medical problems continue to face a different set of rules and risks in the game. Avoiding all infections when possible is not an irrational strategy. But for most of us, a zero Covid strategy just does not comport with family, friends, work, school, and living writ large. For me, a strategy that increasingly accepts the risk of contracting Covid and other infections is necessary for participation in the social world that makes up the fabric of life. But I want to reduce the number of times I contract this disease, and I want to mitigate the potential toll each infection takes in symptomatic or silent ways. I stay up to date with Covid vaccines like the experts tell me to and like the studies continue to show benefit from. I reduce exposures by masking in the office while seeing patients, in planes when traveling, in public bathrooms, and in crowded situations like movie theaters when rates are moderate to high. I test multiple times with symptoms of infection, and treat when positive. And I accept that this approach, these shots, these medications will not work for everyone, nor can they be prescriptions for everyone else’s behavior. I am grateful to be where we are, and I am grateful to watch the science of Covid keep pouring in to review, learn, and teach.
Thank you for reading, and here we go.
Once upon a time I got Covid for the first time. I think.
If you told me at the beginning of the pandemic, when I was trying to keep my head above water and survive a pretty rough situation, feverishly learning about a novel virus late into sleepless nights while trying to protect myself, my family, friends, and patients…. if you told me that it would take almost five years before I contracted Covid, with at least 6 vaccinations in my arm before that illness, and with proven treatment options ranging from antivirals to metformin… I would have taken that deal with exhilaration, and felt like I had cheated the Devil himself.
The story starts out cliched enough. Thanksgiving. People flying in from different parts of the country. Not much ventilation in the house. First: “It’s allergies.” Second: “It’s a head cold.” Third: “My Covid test is positive.” Trust me when I say I started out with a good viral dose of SARS CoV-2 before realizing it was on. Despite being up to date on vaccinations, one of my family members still got quite sick and was in bed for a couple days. The rest have had variable courses.
I don’t personally fear ending up in the hospital or dying. That’s just not my demographic, but developing long Covid is. I’d like to avoid a lingering cough, shortness of breath, fatigue, and especially brain fog and diminution of IQ. I’d also like to reduce the hidden toll that coronaviruses and their spike proteins take on my blood vessels, heart, and brain. Less is more. And so for all these reasons my pregame plan has always been when in doubt, treat. As you might guess, I’m up to date on vaccinations, with the most recent Moderna anti-KP.2 having gone in my deltoid around 9/1/2024.
When I developed a sore throat and nasal congestion with runny nose, I assumed that was Covid. I did not wait for the rapid antigen test to turn positive, as they often are not doing until day 3 or so anyway. Many never turn positive, which is a “good” thing, as it might correlate with low viral loads. But I had my game plan and I was sticking to it. I started Paxlovid. The taste was really gross for me, like sucking on rusty nails with turmeric. I also started metformin, 500 mg on day one. We use metformin for first line treatment of diabetes because it is quite safe, efficacious, and cheap. We also use it in some young women with polycystic ovarian syndrome. I worried that this combination of Paxlovid + metformin might cause some pretty intense gastrointestinal side effects. For me it did not. I started nasal saline rinses using my own technique with a 3 cc syringe. I did these every 2-3 hours. I increased the metformin per the RCT study protocol, and was tolerating 500 mg in the morning, 1,000 mg in the evening within a week no problem. I took meds with meals. I tried to get good sleep, but mostly got my usual 6-7 hours. I took it easy in terms of physical exertion, and mostly stopped exercising. Some people who go on to develop post-exertional malaise and long Covid have been shown to sustain lasting muscle damage with exercising too soon.
Normally with “head colds” and upper respiratory infections I’m sick for a week and then have lasting nasal congestion/sinusitis symptoms that I need to treat aggressively with a couple days of Afrin and a couple weeks of nasal steroid sprays. But with the above regimen of early and consistent nasal saline, an antiviral against the presumed invader, and metformin - I really crushed this. My symptoms remained very mild. I had about 2-3 weeks of unusual fatigue but feel back to baseline now. I have begun exercising again, maybe up to 70% of my usual exertion level. I watch for signs of post-exertional malaise or muscle problems for 3-4 days after each step upwards in exercise intensity. I took a few extra days of Paxlovid beyond the 5.
Hear me when I say that this was my own treatment plan, and I only share it because it worked for me. Anyone reading this should consider it, but ultimately talk to their own doctors about goals of treatment, medication interactions, etc. It felt excessive to me, too. Paxlovid tasted like crap. But then again I have 30 year old patents disabled with long Covid syndromes, sixty year old patients who have had bilateral lung transplants after Covid, older patients with accelerated dementia, cardiovascular disease, strokes, Parkinson’s, and depression after Covid, middle aged patients with new onset cardiac problems, and kids with headaches and new onset “attention deficit” after Covid. I see it.
But don’t take my word for it if you’re part of the crowd that profits financially and politically by denying public health realities. But maybe listen to dispassionate life insurance economists and mathematicians:
The UK and US data shows a large, unexplained jump in deaths attributed to cardiovascular disease (CVD) since 2020. Some countries also reported excess mortality over a pre-pandemic baseline for other major causes of death, such as cancer.
Our general population forecasts suggest that excess mortality will gradually tail off by 2033, to 0–3% in the US and 0–2.5% in the UK. In comparison, by our calculation excess mortality in 2023 was in the range of 3–7% for the US, and 5–8% in the UK.
Official Covid death tolls are only a small part of the whole story. Only chasing Covid hospitalizations and deaths will miss the chance to help billions of other people reduce their risks of long Covid and excess mortality.
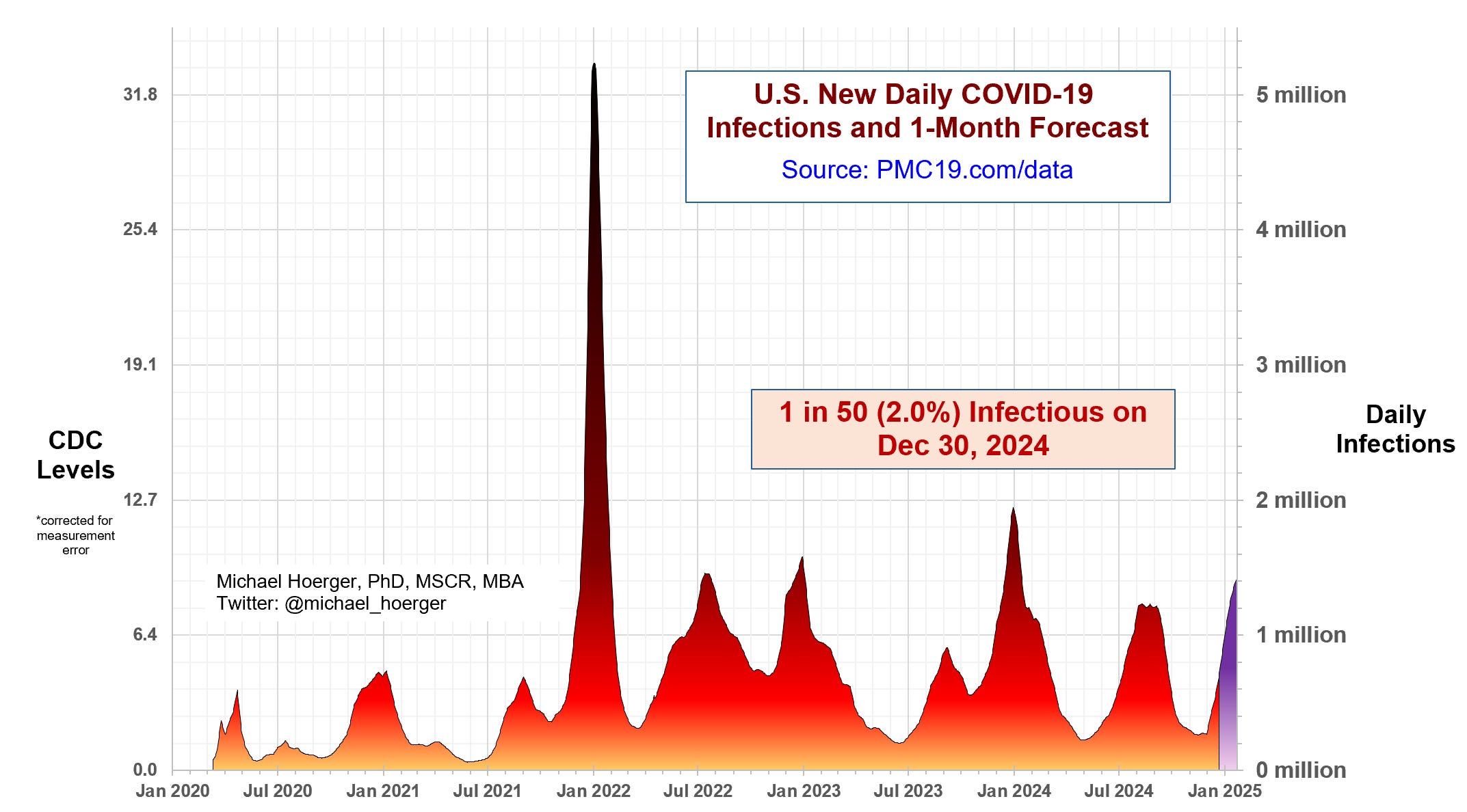
State of Covid
Levels are high after the holidays.
Influenza A, too. RSV, yes.
Here’s the-picture-tells-a-Covid-story, from Pandemic Mitigation Collaborative:
Why are we not using metformin more to treat Covid? It helps.
I think the answer to this question is that metformin is a diabetes medication, and it’s tough for human brains to bend treatment paradigms. But the next time a clinician or online influencer doctor starts talking about ivermectin or hydroxychloroquine, both of which have been proven not to help Covid treatment, ask them about metformin. It should check their boxes (cheap, safe, effective). It has logical mechanisms like anti-inflammatory and antiviral properties. Maybe metformin just lacks a cool, rebellious factor?
In addition to several other studies I’ve highlighted, including the pivotal COVID-OUT randomized controlled trial which showed 40-60% reductions in long COVID risks using metformin, here are two more that escaped me in 2024. These also show impressive results for using metformin with Covid.
Research presented at IDWeek 2024 found metformin prescribed within 6 days of infection reduced long Covid or death by 53% over 6 months in non-diabetic patients. The study used electronic health records to simulate a controlled trial, showing 4.0% of the metformin group developed long Covid/died versus 8.5% in controls. This builds on previous evidence that metformin has obvious potential as an inexpensive, safe treatment option for preventing long Covid.
Another randomized trial (of just 20 people) found that 60% of those taking metformin vs 100% of those given a placebo had detectable SARS-CoV-2 viral loads by day 4 of testing. This comports with previous studies showing one way that metformin works is by reducing viral loads.
Believe it or not, as they say.
Air pollution increases, vaccination decreases long Covid risks
A recent study suggests that exposure to fine-particle air pollution may worsen Covid symptoms and contribute to longer recovery times. The research, published in Environmental Health Perspectives, followed over 2,800 adults in Catalonia, examining factors like air quality, noise pollution, and vaccination status.
Using questionnaires over three years, the study found that about 25% of patients experienced symptoms lasting 3+ months, with increased risks among:
women (27.6% vs 19.4% in men)
those with less education (29.2% vs 22.2% with university education)
those with underlying conditions (33.3% vs 19.7%).
Severe cases had nearly triple the risk of long Covid (71.8% vs 25.1%)
Vaccination provided significant protection, reducing absolute risk from 46% to 15.4%. For those who want to practice their ninja biostatistical analysis tools, that equates to a 67% relative risk reduction in long Covid by being vaccinated.
Some musician entertainers deserve our scorn
A Business Insider investigation revealed that several prominent musicians misused Covid relief funds from the “Shuttered Venue Operators Grant” program for personal luxuries and non-business expenses instead of its intended purpose of supporting live entertainment venues and touring operations.
Money received by individuals:
* Chris Brown: Approximately $5 million personally, plus used $80,000 for birthday party expenses and $24,000 for a non-performance trip to Mexico
* Lil Wayne: $8.9 million grant, with $1.38 million spent on private jets, $460,000 on designer clothes, and $15,000 on flights/hotels for companions
* Marshmello (Christopher Comstock): $9.9 million (entire grant amount)
* Jerry Cantrell (Alice in Chains): $1.4 million
* Sean Kinney (Alice in Chains): $682,000
* Mike Inez (Alice in Chains): $682,000

Teens, preteens, and long Covid
A UK study published in Nature Communications tracked Covid-19 patients aged 11-17 and found that while 70.8% of those with long Covid symptoms at 3 months had recovered by 2 years, 29.2% were still affected. Common symptoms included fatigue, sleep issues, and breathing difficulties. The researchers found no difference in symptoms or their impact based on vaccination status.
The vaccination finding surprised me, as other studies I’ve presented this year found the opposite. I wonder if this failed to show up because the study straddled the time frame when vaccines first arrived? But even if vaccination does not reduce long Covid (contrary to what most other studies have found), then should we be treating kids with some combination of antivirals, nasal saline, or metformin? I can only imagine the backlash such a proposal would unleash among the majority who deny that Covid can bang kids up. See next study below…
More about kids and Covid
A longitudinal cohort study, published in Nature Communications, tracked over 12,000 children and young people in England for 24 months after Covid-19 testing to understand long Covid symptoms. While 25-30% met the research definition of post-Covid condition (PCC) at 24 months, only 7.2% consistently showed symptoms across all time points (3, 6, 12, and 24 months). These persistent cases typically had 5-6 symptoms. Common symptoms included tiredness, sleep problems, shortness of breath, and headaches. Those who were reinfected had more symptoms than single-infection cases. The study found that PCC was more common in older children, females, and those from more economically deprived areas.
For every outlier, there are lots more studies confirming that vaccines do actually help prevent long Covid. Here’s another one in kids.
This one affirms that vaccination does help prevent long Covid in kids, although this study finds that simply reducing infections might be the mechanism.
Published in The Lancet eClinical Medicine, researchers analyzed data from 20 U.S. health systems and found that the Pfizer vaccine was highly effective at preventing long Covid in children and adolescents, with 95.4% effectiveness during the Delta variant period and 60-75% during Omicron. A major difference, and a much better quality study design than above!
But researchers surmised that the vaccine's primary benefit in preventing long Covid came from reducing initial SARS-CoV-2 infections rather than modifying disease course after infection. The findings, which analyzed over 386,000 children and adolescents in three cohorts between 2021-2022, underscore the importance of vaccination as a key strategy for preventing long Covid by reducing infection risk.
I’m drinking the science-flavored Koolaid, and keeping my child up to date with vaccinations until something proves more harm than benefit.
Another study supports kids getting Covid vaccines
A Kaiser Permanente study, published in JAMA Open Network, found the updated XBB Covid vaccine given last year was 65% effective overall in preventing severe outcomes among children 5-17 years old during the 2023-24 respiratory virus season. The vaccine showed 68% effectiveness in ages 5-11 and 63% in ages 12-17.
Uptake remained low at around 7% of kids receiving the shots.
Speaking of kids, they are in trouble, as pediatrician workforce dwindles
STAT news published an excellent article that highlights the after-effects of the pandemic upon our physician workforce. Pediatric medicine is facing a staffing crisis, with 30% of residency programs unfilled and severe shortages across subspecialties, particularly in developmental-behavioral, neurology, genetics, and child psychiatry where over 40% of hospital positions are vacant. The crisis is exacerbated by political factors, including limited support for child-focused legislation, inadequate Medicaid funding for children's healthcare (only 17% of $800 billion Medicaid dollars spent in 2022), and chronic underfunding of pediatric medical education. The situation has led to hospital closures, a 20% decrease in pediatric inpatient units nationwide, and declining interest in pediatric medicine among medical students, with applications dropping 6% this year.
Hug your local pediatrician (and family doc), and let them know you understand the pressures they are experiencing. Then don’t support politicians and DOGE people who want to zero out Medicaid dollars, as this will further wreck the system, even if you have money.
Statistical modeling on when to get a Covid shot
Your Local Epidemiologist highlighted a really interesting study for those of us who try to game out when to get our Covid shots. The best answer is a flexible one that includes current estimates of how much Covid is in the community, upcoming trips and social activity, and how long it’s been since our last infection/vaccination. But if we are just geeking out with the math:
Researchers analyzed optimal Covid vaccination timing by combining projected seasonal incidence patterns from 12 Northern Hemisphere locations with detailed antibody waning and reinfection probability data from both SARS-CoV-2 and related coronaviruses. Their methodology incorporated both seasonal infection risks and vaccine-induced protection levels, which peak in the first month post-vaccination before declining over subsequent months. They calculated cumulative yearly infection probabilities for each possible vaccination date, identifying optimal timing by determining which date produced the lowest probability of infection over the following year.
The fancy computations showed that vaccination should mathematically occur about 2.7 months before anticipated seasonal infection peaks in a given location, allowing peak vaccine protection to align with periods of highest transmission risk. That means like September 15, on average! I don’t think this works well if sending a kid back to school in the middle of a decent wave like this year, though. We got ours the last day of August or so.
But what about timing after infections?
came up with this graphic based on the study, which I will include here but point you back to her site for credit!
Many nursing homes fail to vaccinate seniors, or seniors fail to accept a boost
Nursing homes are struggling with low Covid-19 vaccination rates among residents, with only 40% receiving updated shots during the winter of 2023-24. These are the most vulnerable patients for many reasons. The challenges stem from billing complexities after federal funding ended and increasing vaccine skepticism. While some facilities like Sanford Health achieved high vaccination rates through trusted doctor relationships, many homes face ongoing difficulties protecting their vulnerable populations. Tragic in my opinion.
Spike proteins in the brain after Covid
This next study demonstrates why Covidandia keeps going. We would be foolish to move on from this disease as if it is no longer “novel” or “just like a cold.”
Research published in Cell Host and Microbe found that SARS-CoV-2 spike protein persists in the skull, meninges, and brain of Covid patients long after viral clearance. Using advanced imaging techniques, they detected spike protein accumulation in these areas in both humans and mice. The protein alone was sufficient to trigger neuroinflammation and anxiety-like behavior in mice, and it exacerbated outcomes in brain injury models. The study also found elevated neurodegeneration markers in cerebrospinal fluid from long Covid patients.
While mRNA vaccination reduced spike protein accumulation after infection, it did not completely eliminate it. These findings suggest persistent spike protein may contribute to long-term neurological symptoms of Covid.
Further examining the several different groups of patients that were studied:
Acute Covid patients: These were patients who died of the illness (they examined post-mortem samples)
Non-Covid deaths during pandemic (2021-2022): Skulls from 34 people who died from other causes during the pandemic period, finding spike protein in 10 of these samples - suggesting some had previously had Covid and retained spike protein
Long Covid patients: This group was only studied through cerebrospinal fluid (CSF) samples (not post-mortem tissue), obtained through spinal taps.
So the main tissue proof (spike protein in skull/brain) came from deceased patients, who died from acute Covid or other causes. The long Covid patients were only studied through CSF samples while living, not through tissue examination.
I’ll remind readers that a previous study I highlighted suggested vaccine effectiveness against long Covid/post covid conditions for 1 dose, 2 doses, and 3 or more doses was 21%, 59%, and 73%, respectively. I keep up to date with shots as you know.
And before the mRNA conspiracy kicks in I should add that getting a bunch of spike from vaccination seems much preferable to the whole package with viral infections. Researchers are less concerned about vaccine-induced spike proteins accumulating in the brain because the mRNA vaccines produce a controlled, limited amount of spike protein that stays primarily at the injection site and in nearby lymph nodes, whereas SARS-CoV-2 infection leads to widespread viral replication and significantly higher spike protein levels throughout the body, including mechanisms for viruses directly accessing the brain.
And in the retina…
If we look, we find with this damn disease. Research demonstrates that SARS-CoV-2 can productively infect the retinal pigment epithelium (RPE), causing cellular damage and inflammatory responses similar to age-related macular degeneration, which suggests potential long-term impacts on vision in Covid-19 patients. Published in Proceedings of the National Academy of Sciences.
Another ~30% reduction in long Covid for those receiving at least 3 shots seen
I keep feeling the need to highlight studies consistent with the narrative that staying up to date with Covid vaccinations makes intuitive and demonstrable sense. So here’s another one from this month.
This Hong Kong survey study of 1,542 people, published in Cambridge Press Epidemiology and Infection, found that three vaccine doses reduced the odds of long Covid by 31% compared to two doses, with similar protection from both mRNA and inactivated vaccines used overseas.
Overall, 40.9% reported long Covid symptoms, primarily brain fog (25.9%) and fatigue (20.4%). This 40% is on the high end compared with most studies, so take that with a grain of salt. Also recall that long Covid is not necessarily permanent. But the risk of long Covid was higher among older adults, women, and those with severe initial symptoms. Three doses of Pfizer reduced risk by 32% while Sinovac (China’s vaccine) reduced it by 43% compared to just two Pfizer doses.
Keep a wary eye on H5N1 bird flu
The same stuff we’ve learned and affirmed in Covidlandia this year will apply to the creeping potential disaster brewing right now in the realm of bird flu. More cases identified this week, with more mutations signaling the virus is adapting within human hosts. It only takes one jackpot mutation in one person that hops out of the human incubator and onto the world stage… especially when we are trapped with new public health leadership that defies the sound science of vaccination, masking when needed, or even continuing to fund infectious disease research or pandemic preparedness programs.
This was my primary care take on H5N1 from a couple weeks ago. It went a little viral, as much as I hate that term.
Summary
In the spirit of staying together as human beings in a 2025 world that will seek to further divide us, I’m going to summarize this month’s Covidlandia edition using WE as often as I can.
We saw that current Covid rates are high and climbing through the holidays. Predictable, and so far less coupled with severe disease than previous years it seems (?). And yet Covid death rates are much too high considering how many could have been prevented with some residual caution, additional vaccinations, and antiviral treatment.
We read a case report about a first Covid infection after nearly 5 years of avoiding it, despite being vaccinated and taking precautions. Thanksgiving, of course. My personal treatment protocol included Paxlovid, metformin, and nasal saline rinses, which helped crush developing symptoms effectively, with no lingering concerns as of this writing. I’m still being cautious resuming exercise, which is a good excuse for hurkle durkle and naps.
We saw multiple studies supporting metformin's effectiveness in treating Covid-19, including reducing long Covid risk by 53% when prescribed within 6 days of infection.
We learned that recent research shows air pollution may worsen Covid symptoms, while vaccination significantly reduces long Covid risk (67% relative risk reduction).
We discovered several studies on children and Covid revealing:
About 29% of young people who developed long Covid still had symptoms after 2 years in one study. The overall rate of long Covid happening in kids has been estimated to be somewhere between 5-20%, a wide range reflecting uncertainty and some denialism.
Updated vaccines showed 65% effectiveness in preventing severe outcomes among children 5-17.
Vaccine uptake remains low at around 7-10% of children.
We read about new research finding SARS-CoV-2 spike proteins can persist in the brain and skull after infection, potentially contributing to long-term neurological symptoms. Vaccination helps reduce but doesn't completely eliminate this risk.
We learned the pediatric healthcare system is facing significant challenges, with 30% of residency programs unfilled and severe shortages across subspecialties.
We saw mathematical modeling suggests optimal Covid vaccination timing is about 2.7 months before seasonal infection peaks, but should be adjusted based on previous infections and upcoming situational risks
We read about current concerns including low vaccination rates in nursing homes (only 40% received updated shots) and ongoing monitoring of H5N1 bird flu mutations that could potentially lead to human transmission.
A little thank you gift, from me to you
Here is that 7 page booklet written in outline form of take home points from 12 lengthy Covidlandia posts this year — distilled down into a handy PDF.
Feel free to share it.
I hope it serves you well!
An epic gallery of original paintings, as created by the Examined Artists-in-Residence







Many thanks for brightening up these otherwise gray posts about an uninspiring virus we all resent! There is much beauty still left in the world.
Last post of the year
Many thanks for your support, kindness, and trust.
I’ll keep these coming, if you want.
Take good care out there, and Happy New Year 2025!
~Ryan
Please keep them coming! Covid is changing but it's not going away--but information about it is dwindling.
I'm so glad you utilized your plan and have come through this. Wondering if your test ever turned positive.
It's like flu now--where even uptodate says (re: flu) don't wait for the fairly useless rapid tests--treat if clinical suspicion is high.
Your approach to avoiding infection while living life is just so spot on--and it's just so helpful as we navigate the new normal of an infectious disease that knows no seasonality yet.
Personally, I look at JWeiland and the PMC model (weekly) to get a sense of circulating levels and weigh my own risks/benefits.
I just tried to reach out to a high risk patient who was seen in the ED, actually diagnosed with Covid and sent home with no Paxlovid...it's the norm but why?
Thank you for all you do and please thank the artists.
This is a marvelous summation of our current situation. Thank you again for being the voice of reason in a wasteland of profiteering and politics.