



Covidlandia begins again, January 2025
A review of good stuff from last month

Welcome back to some monthly highlights from a place I call Covidlandia, a forgotten land between black and white, carefree and cautious, pandemic beginning and end. Here I present recent news, scientific discoveries, and medical knowledge that caught my attention and that is of interest to primary care. I try to curate and comment, and realize that one human being cannot possibly keep up with everything. But I try to collect useful, actionable stuff. Twelve editions from 2024 are still relevant. And so we begin 2025. This one takes about 12 minutes to read, so budget that and come back if you want.

I once thought of using a catchy phrase to go with this series, like Keep Covidlandia Weird. You know, like Portland, Oregon’s controversial slogan Keep Portland Weird? But there’s nothing weird about still paying attention to Covid-19, H5N1, and the viral rest. Plus, after the last election even weird has a new connotation.
So if there’s a motto to be had, perhaps in these destructive times targeting science and health communication, I’ll go with:
Covidlandia - truth spoken to power and patient.
~
What’s the current scenario?
Covid rates are improving, though we are still seeing a lot in our office. I’m prescribing Paxlovid when people want it, and offering metformin to reduce long Covid risk. I counsel about possible gastrointestinal side effects and the rest.
I’ve gone back to masking in some situations given high Covid and flu rates, but take my chances in others. It’s my choice weighing the social versus health costs, but I always wear a good mask in the office while seeing patients - for them and for myself.
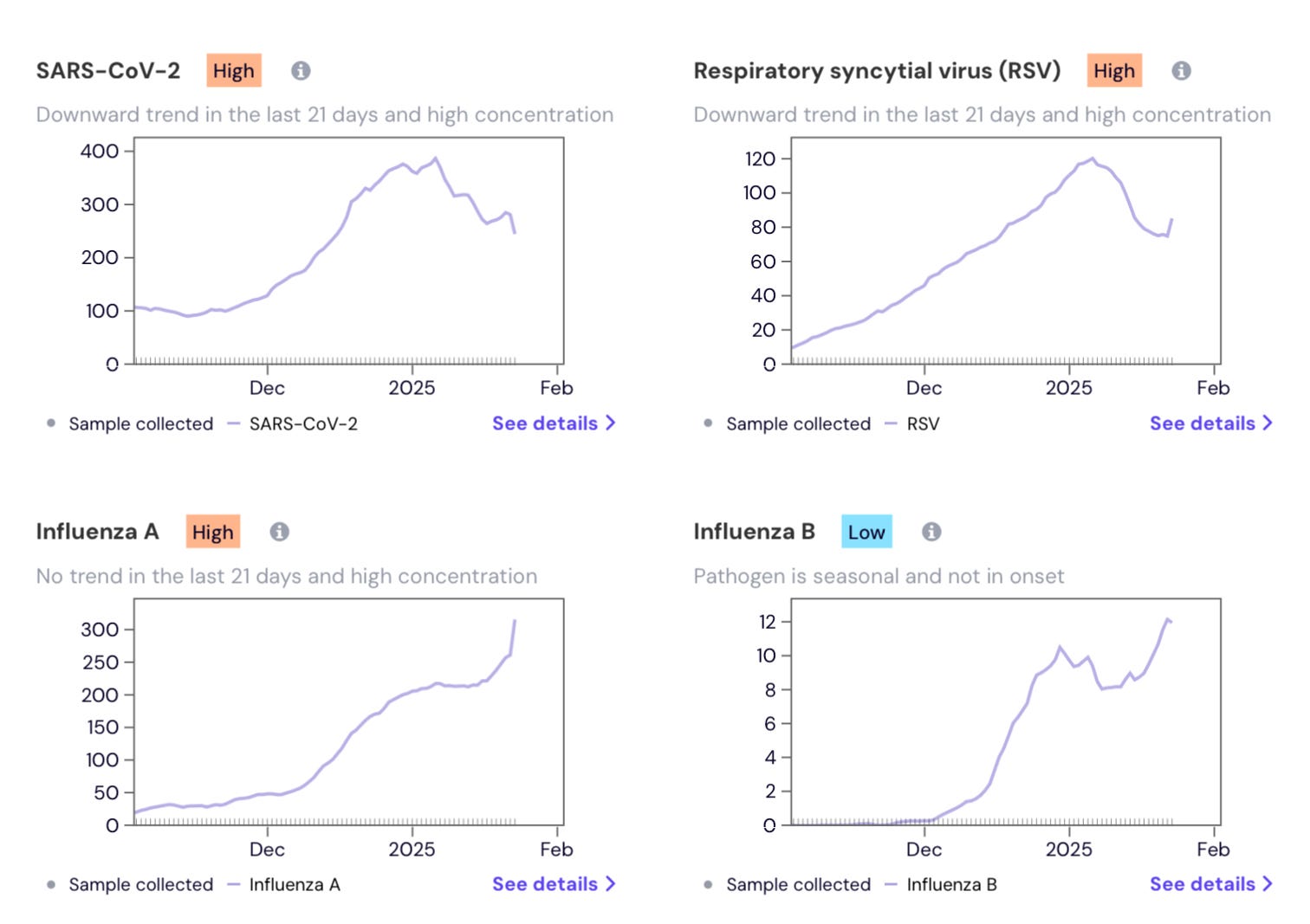
These graphs from WastewaterSCAN help us gauge the national situation. Note that the Y-axes are on different scales, so even though it looks like influenza B is bad, it is still 30-fold lower in wastewater concentration than influenza A.
Covid is taking its damn time improving:
I’ve been getting steady calls, visits, and messages from patients about flu and Covid since the holidays. I know one of my patients is hospitalized with Covid and is receiving remdesivir IV right now. Others are experiencing anything from “allergy symptoms” to “104 fever.” Such a spin of the wheel each time.
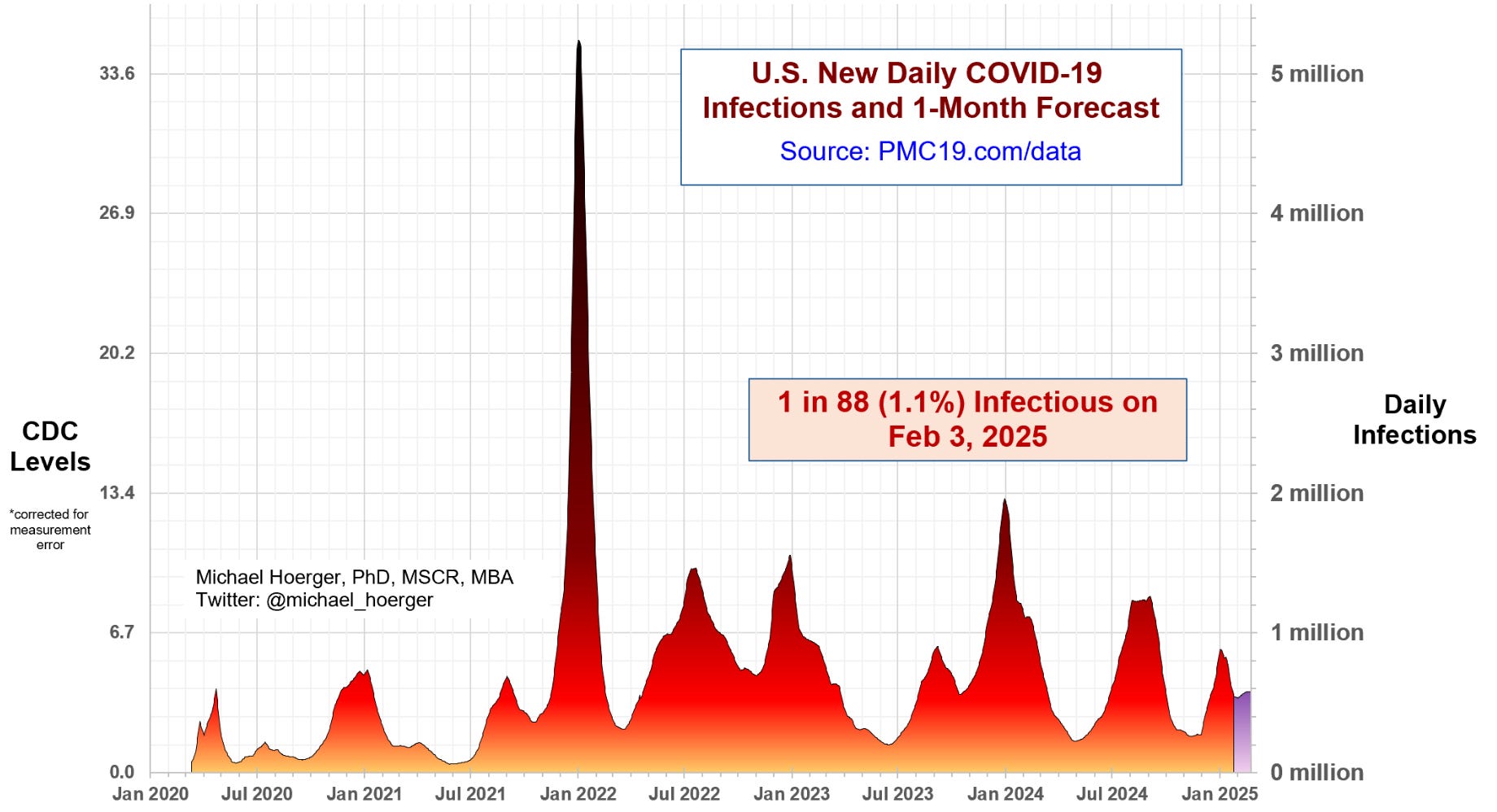
In terms of waves as graphed by the Pandemic Mitigation Collaborative, we can estimate that about 1 in 88 people are infectious with Covid right now:
Would you spray antibodies up your nose twice a day if it gave you 80% protection against contracting Covid?
A fascinating article was published in Science, and buried within it was an even more fascinating hope for future Covid prevention. Researchers identified SA55, an antibody showing promise against current and future SARS-CoV-2 variants, by studying people who recovered from the original SARS virus back in the day, and then later received Covid vaccines. Sinovac Biotech developed it into a nasal spray that showed 80% efficacy in preventing infections. The spray has been used by 300,000 people in China under compassionate use protocols, and while the study has not been officially published, the candidate nasal spray is reportedly in phase 3 clinical efficacy trials now.
I would consider using that before higher risk social activities. Will wait for more data.
Metformin as a Covid treatment
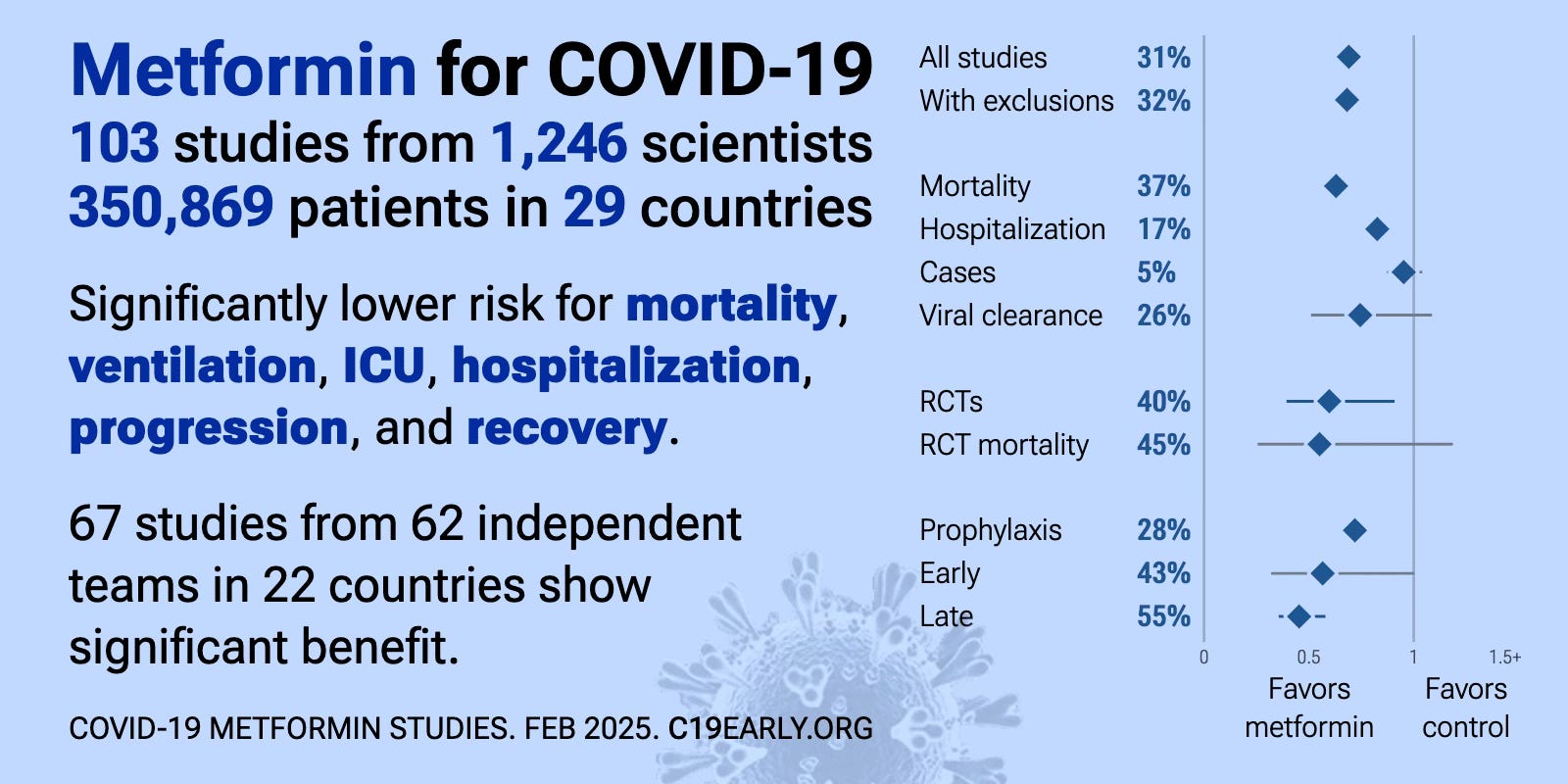
Some doctors have called metformin “the poor man’s Paxlovid” for pretty good reason. It’s cheap, generally well-tolerated, and more evidence keeps piling up that it helps. I highlighted the best studies in my self-treatment plan for Covid post, but a reader named Tara hooked me up with this excellent compendium of 103 other studies (of varying quality, design, and location) that keeps looking good.
According to research examining Metformin's effects on Covid, data from these 103 studies involving 350,869 patients across 29 countries indicates significantly lower risks for several outcomes including mortality, need for ventilators, ICU admission, hospitalization, disease progression, and recovery among patients treated with Metformin. This is in addition to the reduction in long Covid rates I have previously highlighted from RCTs.
The politicization of public health and healthcare
I wrote a note over the weekend about how disturbing the new administration’s silencing and freezing of health agencies and communication has been. It was read by ~7K people (who gave me 1.6K thumbs up and over 230 amazing comments of support). That bolsters one’s spirits. A sincere welcome to you 249 new subscribers, too. Here’s the original note, but I’ll condense the main points as follows:
The systematic dismantling of American public health institutions over the past two weeks demands attention, despite some requesting I write "uplifting" content instead. To do otherwise would turn a blind, cowardly eye to what’s happening in our country. None of us should be doing that. Truth must be spoken to power and patient alike.
Recent alarming developments include:
Federal health agencies (CDC, FDA, NIH) forced to halt external communications, with critical resources like Vaccine Information Sheets that I use every day vanishing, and some H5N1 outbreak data gone
Scientific meetings and research panels abruptly cancelled, crippling ongoing studies and clinical trials
All public health communications now require political approval
Collaboration with WHO halted during crucial, present H5N1 bird flu concerns
Government-wide hiring freeze and worker intimidation implemented
The nomination of RFK Jr. for HHS Secretary still alive, despite his well-documented history of vaccine misinformation for ongoing profiteering
All of this isn't mere disruption - it's destruction aimed at centralizing power at truth's expense. We can only hope for some luck, some bravery, some awakening.
Some regret.
Mainstream media sources that document the above: [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11][12] [13] [14]
This year’s updated Covid shots are working well
Did you get your annual Covid shot, like your annual flu shot? I did.
A study just released from the VA Healthcare System looked at the current 2024-2025 Pfizer COVID-19 vaccine’s effectiveness:
The study evaluated vaccine effectiveness among 44,598 respiratory infections between September-November 2024, providing robust data on real-world performance of the updated Pfizer formulation.
The vaccine showed strongest protection against severe disease, demonstrating 68% effectiveness in preventing COVID-19 hospitalizations.
For preventing emergency department and urgent care visits, the vaccine was 57% effective
In outpatient settings (my primary care world), the vaccine showed 56% effectiveness at preventing COVID-19 visits.
But despite these positive effectiveness findings, the researchers noted that uptake of these updated vaccines remains low among the population.
Since this study was conducted within the VA Healthcare System, results may differ in other populations. Additionally, longer-term effectiveness data would be needed to assess durability of protection.
Updated vaccines are the victim of conspiracy theories and even low doctor enthusiasm. But based on the above data, and the data for every additional Covid shot so far, the logical conspiracy would, however, go like this:
You’re just telling me to get this updated shot so that your office will have less Covid visits, your health system less urgent care and ER visits, and your hospital less Covid admissions - all of which adds up to millions of dollars of lost revenue!
To which I would answer: That’s right, plus less long Covid and other cumulative stuff. Maybe try Novavax if you react strongly to mRNA. Read on.
Immunodeficiency from COVID
I read at least three articles this month on the taboo subject, one that you definitely will not hear from any folks telling you that Covid is just a cold. Sometimes it is, and sometimes it isn’t. We need to keep living our lives, but I bend the percentages when I can to avoid or at least treat Covid in my life.
Synthesizing this study in the journal Science, with this article from The Sick Times, with this post from LIL Science, I can present the following take home points about immunodeficiency.
The relationship between COVID-19 and immune system dysfunction is more complex than initially understood. Recent research with 113 patients revealed that Long Covid involves specific damage to complement and coagulation systems, creating microclots and inflammation. However, early attempts to characterize this immune damage led to two problematic narratives.
First, some advocates drew parallels to HIV/AIDS, but this comparison is scientifically inaccurate. While HIV directly targets and destroys T-cells, COVID-19 affects cells differently, though both diseases faced similar patterns of public health minimization and stigmatization.
Second, the theory of "Immunity Debt" emerged, incorrectly suggesting that isolation during the pandemic weakened immune systems. This has been disproven by data from Sweden, where minimal lockdowns still led to severe respiratory virus seasons. Instead, evidence points to COVID-19 itself causing immune dysfunction through multiple mechanisms, including reduced T-cell counts and altered immune responses.
Understanding these distinctions is crucial for developing targeted treatments and implementing effective prevention strategies. The science suggests focusing on preventing COVID-19 infection and utilizing treatment, rather than worrying about immune system "debt" from isolation.
A great zoomed out article about lessons learned during the pandemic
Writing for STAT News, Helen Branswell reflected on lessons from the Covid-19 pandemic five years after its emergence. Key takeaways include:
Public trust in health institutions like the CDC has significantly declined due to communication missteps and policy changes, many of which were fumbled for logical reasons in real time with impossible to balance competing prerogatives.
mRNA vaccine technology proved revolutionary but faces growing public skepticism. Nothing comes close to the speed and precision this technology affords to respond quickly to novel pathogens. (Plus, relying on old production techniques involving chicken eggs might be completely disastrous in an H5N1 bird flu pandemic that has already slaughtered 150 million chickens.
While non-pharmaceutical interventions (like masks and school closures) were effective to stop the bleeding, political divisions and new legislation may make these measures harder to implement in future pandemics. She warns that these factors could cripple a response to the next pandemic.
An H5N1 pandemic would be expected to flip the demographics, with children and young adults often at highest risk during flu pandemics.
Since this article was written, we are now very close to a dream team (nightmare) of Robert Kennedy Jr., Marty Makary, Dave Weldon, Mehmet Oz, and Jay Bhattacharya leading our country’s health institutions.
Between burnout, opaque leadership, and self-preservation instincts, we should anticipate the healthcare workforce would crater in the event of an even more lethal pandemic 2.0. Follow the links if you don’t believe me.
Air filters can help
In addition to cracking some windows and getting fresh air into whatever building is hermetically sealed, air filters can help.
A new review in Journal of Infection and Public Health found that portable air filters (PAFs) reduce infections from airborne diseases. “This is settled science, and has been for decades,” the authors wrote, highlighting that portable purifiers had many benefits besides filtering airborne viruses, including filtering allergens and wildfire smoke.
For instance, Myers et al., [10] sampled air from the rooms of patients with newly diagnosed COVID-19. They found that 44% of air samples in rooms with sham PAFs without filters tested positive for coronavirus RNA. This decreased to 25% in rooms with operational PAFs running at their lowest settings.
The authors recommend that public health authorities “position PAFs appropriately in infection prevention and control plans for both health care and community settings in order to more effectively address airborne infectious diseases.”
Another antiviral medication against Covid?
A study published in Nature highlighted a promising new treatment option for Covid. The drug is called azvudine, and was first discovered in 2007 as a hepatitis C treatment. It was later developed for HIV and Covid, receiving Chinese approval for both conditions by 2022. A recent large-scale study of 40,876 hospitalized Covid patients found azvudine reduced death risk by 18% compared to Paxlovid, with fewer adverse events. The drug works by inhibiting viral RNA replication.
A good review and impetus to keep people on their statins during and after infection?
The American Heart Association News published a good primer on how Covid can harm blood vessels and the heart. The coronavirus enters cells through ACE2 receptors and hijacks cellular mitochondria, potentially triggering an excessive immune response called a cytokine storm. This can lead to inflammation in blood vessels and heart tissue, increasing risks of heart attacks, strokes, and myocarditis. While these risks may decrease over time as immunity builds, vulnerable populations remain at higher risk.
In my self-treatment plan for Covid I’ve mentioned that keeping patients on a statin during Covid may prove beneficial to mitigate some of this inflammation in coronary artery plaque. Many statins cannot be take with Paxlovid, but pravastatin can. It costs about 25 cents a pill, so I often discuss this substitution for 7 days in people taking rosuvastatin or atorvastatin.
Better to be vaccinated against Covid
In this VA study of 141,520 total patients (68,581 in 2022-23 season, and 72,939 in 2023-24 season), published in JAMA Internal Medicine, researchers compared outcomes of non-hospitalized veterans who were tested for COVID, flu, and RSV on the same day.
Among unvaccinated patients, COVID-19 showed higher 30-day hospitalization rates (17.5% in 2022-23) and 180-day mortality (3.1%) compared to flu and RSV.
However, in vaccinated individuals, there was no significant difference in hospitalization or mortality rates between COVID-19 and flu patients during either season, demonstrating vaccination's effectiveness in reducing COVID-19 severity to levels similar to seasonal flu.
Updated Covid vaccines are still safe
A study of 7.6 million Medicare beneficiaries aged 65+ who received 2023-2024 COVID-19 vaccines found no major safety concerns. While a rare potential increase in anaphylaxis risk was observed with Pfizer-BioNTech's vaccine, no other significant health risks were identified. Most recipients received either Pfizer (48.8%) or Moderna (50.8%) vaccines, with Novavax coming in at a very distant 3rd (0.40%).
There is always the risk of adverse reactions with any shot, but in terms of risk/benefit, this analysis is reassuring. It is also possible that people who react most strongly to the mRNA shots are not keeping up any more. For these sorts of folks who still want a vaccination, I recommend Novavax. It is better tolerated with less side effects, and seems to work about as well. This was a great Novavax deep dive by Ed Nirenberg that I previously linked to.
Can Paxlovid treat Long Covid?
This question has not been definitively answered yet. One RCT I wrote about last year found not much benefit, but it was imperfectly designed. An interesting case series was published last month in Nature Communications, looking at 13 individual stories of patients with long Covid who were treated with Paxlovid for varying durations, with some mixed results. Case series are of low scientific authority. But it’s worth a look, and it’s worth continuing to study Paxlovid as a treatment for long Covid. Plus, stories are more interesting than data to the human mind.
Results were decidedly mixed: Out of 13 stories, nine patients reported some improvement, but only five said it lasted. Four reported no improvement at all.
In the future I think Paxlovid will be proven to have some limited benefit in certain patients who have not fully cleared the virus. The duration of therapy needs to be worked out, and I’m guessing the earlier a patient tries an extended course of treatment the greater the chance of success.
I’ll add one more story. Sometimes I discuss trying Paxlovid with patients seeing me for long Covid. I present the unknowns. One 58 year-old patient was suffering brand new, daily, moderate to severe headaches for 6 months after his first Covid infection. He took a course of Paxlovid for 5 days. His headaches resolved within a week and it has now been over a year since that time, and no headaches returned.
Some other patients I could report had no such luck, and for some others there have been mixed results.
Paxlovid and kidney disease
A study published in Open Forum Infectious Diseases found that Paxlovid reduced hospitalization, major cardiovascular events, and death in COVID-19 patients with kidney disease. Among 1,095 treated patients versus 584 untreated, those receiving Paxlovid had lower 30-day hospitalization rates (3% vs 8%) and lower one-year mortality.
Is what works for the goose often good for the gander? Even if we don’t have kidney disease, would the same viral load-reducing mechanisms of antiviral medications help reduce our long terms risks each time we get Covid?
Previous studies also showed accelerated kidney function decline after serious Covid illness, worse than what happens with pneumonia.
One more in support of Paxlovid
Another large, real-world study (published in PLOS Medicine) of over 700,000 COVID-19 patients found Paxlovid significantly reduced negative outcomes when given within 5 days of infection. The medication lowered hospitalization risk by 39% and death risk by 61%, benefiting both vaccinated and unvaccinated patients. However, disparities in access were noted, with Black and Hispanic patients (around 15%) receiving Paxlovid less frequently than White and Asian patients (around 23%).
Both 15% and 23% suck in my humble opinion. One of my patients told me this week that her 87 year old mother almost died of Covid. Her doctor also told her that Paxlovid was not worth it since she wasn’t feeling so bad at that moment.
Will regular flu shots help us in the event of an H5N1 bird flu pandmic?
With egg prices soaring, and hens everywhere being slaughtered, it is a grim time to be a chicken. I wrote a post about prepping for an H5N1 pandemic that was pretty well read. I’d like to add this bit of real world evidence to answer the question of whether regular flu shots might offer us some cross-protection against bird flu.
A study published in mBio investigated whether seasonal flu vaccines could provide protection against potential avian influenza (H5N1 and H7N9) pandemics. Researchers analyzed blood samples from 135 Spanish individuals across three age groups, before and after receiving seasonal flu vaccines. They found that baseline protection against these avian flu strains was very limited in the population. However, seasonal vaccination did increase protective antibody levels against H5N1 in about 15% of younger participants, though this protection largely disappeared after six months.
Examining the data from the paper, for H5N1 protection after seasonal vaccination:
Younger group (born 1978-1997): 15.0% developed protection
Middle group (born 1968-1977): 12.2% developed protection
Older group (born 1925-1967): 0% developed protection
The older group (G1) showed no seroconversion response against H5N1 after vaccination, which the authors suggest might be due to immunosenescence (age-related decline in immune function). This is particularly noteworthy since the older group actually received a high-dose version of the quadrivalent flu vaccine, while the younger groups received a standard-dose version.
Overall the study suggests that seasonal flu vaccines could serve as a shaky first line of defense during the early stages of an avian flu pandemic when specific vaccines are not yet available, but would need to be followed by strain-specific vaccines for better protection. Often younger people are more severely effected by influenza pandemics, so a flu shot would be especially important for them (?).
Also be aware that in the final days of the Biden/Harris administration, Moderna was awarded $590 million to develop mRNA vaccines targeting potential pandemic flu threats, particularly H5N1 and H7N9 avian influenza strains. The project includes clinical trials for multiple flu variants and aims to enhance pandemic preparedness using mRNA technology. Thank you for your service.
Conclusion
We made it. The first Covidlandia installment of 2025. Thanks for you support and readership. Here’s what we learned and reviewed:
Current COVID Scenario: rates are improving but still present at pretty high levels, like 1 out of every 88 people potentially infectious.
Nasal Antibody Spray: shows 80% efficacy against Covid transmission in Chinese trials. More work to be done
Metformin: Analysis of 103 studies confirms metformin's effectiveness as a low-cost Covid treatment, reducing multiple negative outcomes.
Public Health Politicization: Major disruptions in federal health agencies including communication freezes and resource removal are raising serious concerns.
COVID Shots: VA study shows the current 2024-2025 vaccine is significantly effective, with 68% protection against hospitalization.
Immunodeficiency: Research reveals Covid causes specific immune system damage, distinct from previously assumed "immunity debt."
Pandemic Lessons: Five years into the pandemic, key challenges include declining public trust and political divisions affecting response measures.
Air Filters: Research confirms portable air filters significantly reduce transmission in indoor spaces.
Azvudine: New antiviral shows 18% lower death risk compared to Paxlovid in large study.
Cardiovascular Effects: Covid can damage blood vessels and heart, with statins potentially helping to reduce inflammation.
Vaccine Effectiveness: VA study shows vaccinated individuals have similar Covid outcomes to flu, while unvaccinated face higher risks.
Paxlovid Research: Shows mixed results for Long Covid but clear benefits for kidney disease patients and general Covid treatment
H5N1 and Flu Shots: Seasonal flu vaccines might offer limited cross-protection against H5N1, mainly benefiting younger populations temporarily
Take good care!
I am so grateful when you write. I also admire your clear way of summarizing results from diverse sources. You make such a difference in many lives.
Thank you!
I have a quick question - is it okay if I share your original "politicization of healthcare" article?
Also, your resident artist continues to astound me!! What a beautiful picture. I hope she loves what she does and will keep expressing herself and sharing her precious gift with the world. It makes me think of the old Dostoyevsky quote, "the world will be saved by beauty", (and of course by truth - thank you for that!).